EMDR Explained: The Neuroscience Behind Why It Works

It probably comes as no surprise that I have a deep fascination with the human brain and how different therapeutic approaches can change it. The idea that a structured intervention can physically alter neural pathways in our brain, shift stress responses, and dissolve long-held behavioural patterns is, to me, fascinating. The topic I will talk about today is EMDR, as not only is it an incredible therapeutic modality, but the science behind it is also extraordinary.
This post covers quite a bit of ground: what EMDR actually is, how a session is structured, and what the neuroscience tells us about what is happening in the brain during and after treatment, and more. If you have ever been curious about EMDR, I hope this gives you a clearer picture.
What is EMDR?
EMDR which stands for ‘Eye-Movement Desensitisation and Reprocessing’ is an evidence-based form of psychotherapy developed by Francine Shapiro in 1989. It initially focused on treating post-traumatic stress disorder (PTSD), but over time it has been adapted for other issues individuals may be facing such as attachment-focused trauma, addiction, anxiety, depression and chronic pain, and the research supporting these wider applications continues to grow.
How Trauma Memories Are Stored in the Brain
Before going into how EMDR works, it is helpful to understand what is actually going wrong in the brain in the first place.
When a traumatic event occurs, the brain can struggle to process and integrate the experience in the way it would process an ordinary memory. Our everyday memories are stored in a relatively coherent, time-stamped manner. For instance, you know when they happened, you can place them in your life story, and they do not carry the same raw emotional charge as when you first experienced them. Traumatic memories on the other hand, often do not follow this pattern. They can remain fragmented, non-linear, and intensely emotionally loaded. They can surface out of the blue as intrusive images, bodily sensations, or overwhelming emotional states that feel present-tense rather than past-tense.
This happens, in large part, because of what the amygdala and hippocampus are doing under extreme stress (see image 1 for where these regions are located in the brain). The amygdala, often referred to as the brain's threat-detection system becomes hyperactivated and encodes the specific experience with a high emotional charge. At the same time the hippocampus, which is responsible for making sense of memories and placing them accurately in time, is impaired by the flood of stress hormones. The result is a memory that has been stored without a sense of when it happened or where it belongs. It sits, as it were, outside the normal memory filing system, and continues to behave as if the threat is ongoing.
One of the central aims of EMDR is to revisit that memory within a safe, regulated context and support the brain to essentially go back and process it properly.
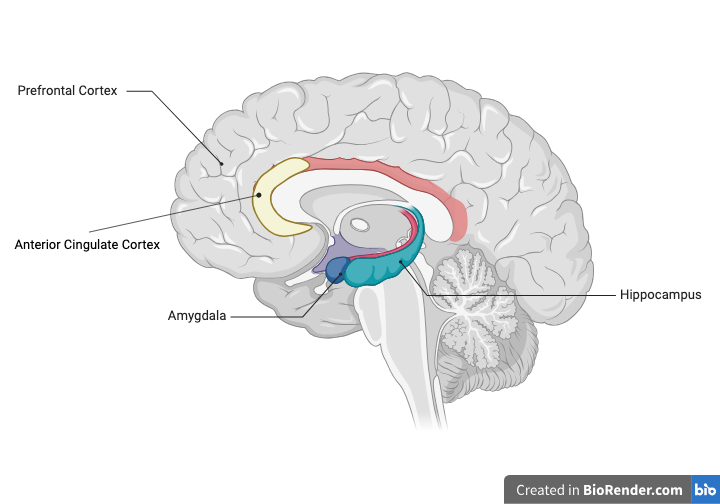
Cross section of the human brain showing the location of brain regions associated with traumatic events and EMDR therapy.
How an EMDR Session Works: The Eight-Phase Protocol
EMDR sessions involve a technique called bilateral stimulation - the rhythmic, alternating activation of both sides of the body through eye movements, tapping, or sound. But bilateral stimulation is just one component of a carefully structured, eight-phase clinical protocol, and understanding that structure goes a long way to explaining why the therapy works as well as it does.
The eight phases move through
· history-taking
· preparation
· assessment of the target memory
· desensitisation
· installation of a positive belief
· a body scan
· closure
· re-evaluation
What this means in practice is that a client is never simply asked to revisit their trauma and hope for the best. They are prepared beforehand, supported throughout, and brought back to a settled state before the session ends. It is worth noting that this protocol has been adapted for use in different contexts- as discussed towards the end of this post and may look somewhat different depending on the presenting needs of the client.
Progress is tracked using two straightforward measures: the SUDS scale, which asks clients to rate their distress from 0 to 10, and the VOC scale, which measures how strongly they believe a positive statement about themselves such as "I am safe now" on a scale of 1 to 7. This allows the therapist and client to track progress over time in a more concrete way.
Bilateral Stimulation: What is Actually Happening?
Bilateral stimulation is what runs through the heart of the EMDR protocol. In simple terms, it means rhythmically activating both sides of the body in an alternating pattern. The client's eyes might follow the therapist's moving fingers or a light moving from side to side, they might receive alternating taps on their hands or knees, or listen to tones that switch from ear to ear. It sounds deceptively simple, but what it does to the brain is considerably more interesting.
Researchers have been trying to pin down exactly why it works for decades, and the honest answer is that there is no single, universally agreed explanation. What we do have is a set of well-evidenced hypotheses that complement each other.
The REM Sleep Hypothesis: Shapiro originally noticed a resemblance between the eye movements used in EMDR and the eye movements that occur during Rapid Eye Movement (REM) sleep- the stage most associated with emotional memory processing. Stickgold (2002, 2008) developed this into a formal proposal: that bilateral stimulation shifts the brain into a similar state, one where the emotional alarm system quiets down and distressing memories can finally be integrated rather than kept frozen in place.
Subsequent research suggested this may unfold in two stages: first, a slower, deeper state that begins to loosen the grip of the traumatic memory, followed by a REM-like phase where it is properly consolidated (Castelnuovo et al. 2017). Put simply, EMDR may be creating the conditions for the brain to finish processing something it never got to complete.
The Working Memory Hypothesis. This is probably the most extensively researched explanation for why bilateral stimulation works. Andrade, Kavanagh and Baddeley (1997) proposed that performing eye movements whilst holding a traumatic memory in mind places a significant demand on working memory - the part of the brain responsible for juggling information in the present moment. Because the trauma image and the eye movements are competing for the same mental resources, the vividness and emotional intensity of the image reduce in real time. Research has since shown that tapping and auditory tones (as an alternative to using side-to-side eye movements) produce the same effect, which is interesting as it tells us that it’s not the eye movements themselves that are doing the work. It is the load placed on working memory that potentially matters.
The Neuroscience: What EMDR Does to the Brain
Neuroimaging research has given us a clearer picture of what EMDR is actually changing in the brain.
Reduced Amygdala Activation: The amygdala, the brain’s alarm system for detecting threats, shows measurable reductions in hyperactivity following EMDR therapy. Boukezzi et al. (2017) found that EMDR normalised amygdala responses to emotional stimuli in PTSD patients, directly correlating with symptom reduction. In short, the alarm system that kept firing long after the danger had passed begins, finally, to stand down.
Increased Prefrontal Cortex Function: At the same time, activity in the prefrontal cortex increases (responsible for rational thinking and emotional regulation). This matters because trauma disrupts the prefrontal cortex's ability to calm the amygdala down. EMDR appears to restore that connection, giving the brain back its capacity to recognise that what happened then, is not what is happening now.
Anterior Cingulate Cortex: Research has also identified changes in the anterior cingulate cortex, a region that acts as a bridge between emotional and rational systems. Pagani et al. (2012) were among the first to capture these changes in real time. Using EEG they observed a change in neural activity away from limbic regions and towards higher thinking areas, as bilateral stimulation progressed. In other words, the memory was moving from something raw and reactive towards something more integrated and resolved.
Hippocampal Memory Processing: The hippocampus also shows meaningful changes following EMDR. It recovers its ability to do what trauma prevented it from doing in the first place- telling the brain that this memory belongs in the past, not the present (Rousseau et al. 2019).
The Somatic Dimension: The Nervous System and EMDR
EMDR is not only a cognitive intervention, but a somatic one also. Somatic simply means relating to the body. Clients are asked to track body sensations throughout the protocol, and the body scan phase specifically addresses any residual physical disturbance before a session closes.
This is an important consideration because trauma does not live only in the mind. When a threatening event occurs, the autonomic nervous system shifts into survival mode (fight, flight, or freeze), and in cases of unresolved trauma, it can remain stuck there long after the danger (or perceived danger) has passed. Successful trauma therapy involves helping the nervous system shift out of that survival mode and back into a regulated, settled state.
What this means in practice is that EMDR is not asking clients to think their way through trauma. It works with the whole system at once: nervous system, body, memory, and cognition together.
After the Session Ends: Why Your Brain May Keep Processing
One thing worth knowing before beginning EMDR is that the processing does not necessarily stop when the session ends. The brain can continue integrating material for hours or even days afterward. New insights may surface, related memories may emerge, or dreams may appear vivid or random. This is not a cause for concern; it is the brain doing exactly what the therapy set in motion.
The reason this happens comes down to what Shapiro called the Adaptive Information Processing model. Traumatic memories are stored in isolated networks, cut off from the broader web of memories, emotions, and meaning that make up a person's life story. EMDR begins to reconnect them. As bilateral stimulation activates the target memory, the brain starts forming new synaptic connections, linking the previously isolated memory to more adaptive information held elsewhere in the neural network. That reconnection process does not always complete within the session itself- the brain continues making those connections afterward, which is why the days following an EMDR session can feel unexpectedly rich with insight, emotion, or clarity.
It is also why the re-evaluation phase at the start of each subsequent session matters. The therapist checks what has arisen between appointments, because what emerges in the days after a session is often as clinically significant as what happened during it.
EMDR Beyond PTSD
While EMDR is best known for its success in treating PTSD, emerging research suggests its benefits extend far beyond trauma-related disorders. Research has shown promising results for anxiety, depression, and chronic pain, and EMDR has been successfully adapted for a wide range of populations including children, first responders, and those with complex or developmental trauma among them.
Attachment-Focused EMDR (AF-EMDR) is one such adaptation, designed specifically for individuals whose difficulties trace back to early attachment relationships such as parental neglect, misattunement, or chronic emotional unavailability. Where standard EMDR places the emphasis on processing a single, identifiable traumatic memory, AF-EMDR places far greater weight on building internal resources first: strengthening a felt sense of safety, self-worth, and connection that early experience may never have provided. It is the internal groundwork that makes the deeper processing possible.
A Note From My Practice
In my own practice, I integrate elements of EMDR-informed technique within hypnotherapy sessions where appropriate - an approach known as Hypno-EMDR, which combines bilateral stimulation with the deeply relaxed, receptive state that hypnotherapy creates. The neuroscience that underpins both modalities is, as this post reflects, something I find endlessly amazing.

References
Andrade, J., Kavanagh, D., & Baddeley, A. (1997). Eye-movements and visual imagery: A working memory approach to the treatment of post-traumatic stress disorder. British Journal of Clinical Psychology, 36(2), 209–223.
Boukezzi, S., El Khoury-Malhame, M., Auzias, G., Reynaud, E., Rousseau, P. F., Richard, J., ... & Khalfa, S. (2017). Grey matter density changes of structures involved in posttraumatic stress disorder (PTSD) after recovery following Eye Movement Desensitization and Reprocessing (EMDR) therapy. NeuroImage: Clinical, 15, 571–580.
Castelnuovo, G., Fernandez-Aranda, F., & Tonioni, M. (2017). Eye movement desensitization and reprocessing and slow wave sleep: A putative mechanism of action. Frontiers in Psychology, 8, 1935.
Pagani, M., Di Lorenzo, G., Verardo, A. R., Nicolais, G., Monaco, L., Lauretti, G., ... & Siracusano, A. (2012). Neurobiological correlates of EMDR monitoring — an EEG study. PLOS ONE, 7(9), e45753.
Parnell, L. (2013). Attachment-focused EMDR: Healing relational trauma. W. W. Norton & Company.
Rousseau, P. F., El Khoury-Malhame, M., Reynaud, E., Boukezzi, S., Cancel, A., Zendjidjian, X., Guyon, V., Samuelian, J. C., Guedj, E., Chaminade, T., & Khalfa, S. (2019). Fear extinction learning improvement in PTSD after EMDR therapy: An fMRI study. European Journal of Psychotraumatology, 10(1), 1568132.
Shapiro, F. (1989). Eye movement desensitization: A new treatment for post-traumatic stress disorder. Journal of Behavior Therapy and Experimental Psychiatry, 20(3), 211–217.
Shapiro, F. (2018). Eye movement desensitization and reprocessing (EMDR) therapy: Basic principles, protocols, and procedures (3rd ed.). Guilford Press.
Solomon, R., & Shapiro, F. (2008). EMDR and the adaptive information processing model: Potential mechanisms of change. Journal of EMDR Practice and Research, 2(4), 315–333.
Stickgold, R. (2002). EMDR: A putative neurobiological mechanism of action. Journal of Clinical Psychology, 58(1), 61–75.
Stickgold, R. (2008). Sleep-dependent memory processing and EMDR action. Journal of EMDR Practice and Research, 2(4), 289–299.