The Neuroscience of Trauma and PTSD
Introduction
One of the reasons that I pursued clinical training after my PhD (and continue to) is my deep fascination with how the brain and body become rewired by experience. Not just traumatic experience, but all of it - the mundane, the joyful, the devastating and everything in between. A question that drives a lot of my work is what happens when this rewiring might work against us – and whether it can be undone.
Trauma is where that question gets interesting. What happens in the brain when an experience becomes traumatic. Why some people develop PTSD while others don’t. Why flashbacks feel so viscerally real, even decades later. And what neuroscience tells us about how the brain can, and does, heal.
What is Trauma?
Trauma refers to a person’s emotional and psychological response to distressing events that overwhelm their ability to cope. Bessel van der Kolk sums it up particularly well: trauma overwhelms the nervous system's capacity to regulate itself, and produces lasting changes in brain structures involved in fear, memory, and executive control - the amygdala, hippocampus, and prefrontal cortex.
But not all trauma looks the same.
‘Big T’ & ‘little t’ trauma
Traumatic experiences range from acute, life-threatening events - such as natural disasters, serious accidents, or personal assaults, to ongoing, less obvious stressors that accumulate over time. When the brain is unable to process these experiences effectively, it can lead to Post-Traumatic Stress Disorder (PTSD), a condition characterised by persistent symptoms such as flashbacks, hyper-vigilance, and severe anxiety.
It helps to distinguish between ‘Big T’ and ‘Little t’ trauma. ‘Big T’ trauma refers to severe, life-threatening events like war, sexual assault, or catastrophic injuries - experiences most directly associated with PTSD. ‘Little t’ trauma, on the other hand, includes chronic stressors such as emotional neglect, repeated criticism in childhood, or workplace bullying. These may not always result in PTSD, they can have a cumulative effect on mental health, leading to anxiety, depression, and nervous system dysregulation over time.
(Side note: Just because something is labelled as 'little t' trauma doesn't make it any less significant or impactful).
What Happens in the Brain During Trauma?
Traumatic events trigger significant changes in the brain, particularly in three key regions involved in stress and memory processing.
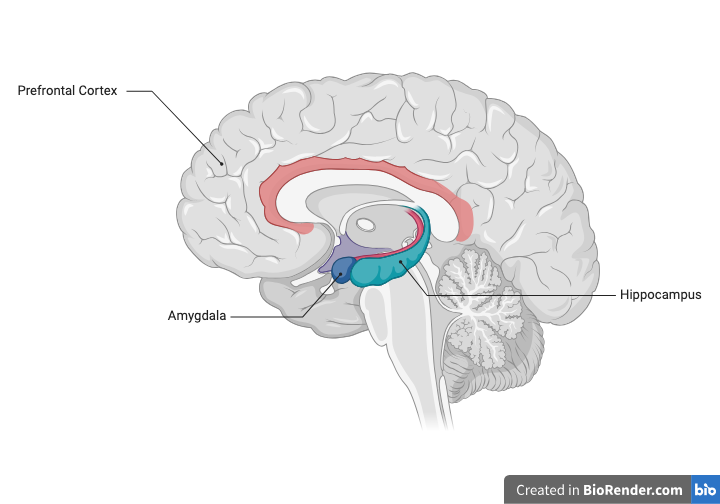
Cross section of the human brain showing the location of the prefrontal cortex, amygdala and hippocampus - three regions central to trauma and PTSD.
The Amygdala, a small, almond-shaped structure, processes fear and activates the fight, flight, or freeze response. In individuals with PTSD, it becomes chronically overactive, generating heightened fear responses even in the absence of real threat. This keeps the autonomic nervous system - the system that regulates heart rate, breathing, and digestion, in a state of persistent alarm, long after the danger has passed.
The Prefrontal Cortex (PFC) is responsible for decision-making and emotional regulation. Under extreme stress or trauma, it can become less active, reducing its ability to regulate the amygdala. This imbalance contributes to exaggerated fear responses and difficulty in controlling emotions and impulses.
The Hippocampus shapes how memories are formed and retrieved. Trauma disrupts this process, leaving memories fragmented, non-linear, or intrusive- which is why flashbacks feel less like remembering and more like reliving. It also explains why trauma survivors giving statements to police may recall events out of sequence. Specialised techniques like cognitive interviewing have been developed precisely because of this.
Why Do Some People Develop PTSD and Others Don't?
This is one of the most important questions in trauma research, and the answer is not simply about the severity of what happened or how strong a person is.
Several factors influence vulnerability. Prior trauma exposure, particularly in childhood, sensitises the body's stress response system, known as the HPA (hypothalamic-pituitary-adrenal) axis, making it more reactive to threat later in life. Genetics also play a role. For example, variations in genes that regulate serotonin and cortisol- two chemicals central to how we handle stress, appear to increase susceptibility (Ressler et al., 2011). And brain structure itself matters. Research has found that individuals with a smaller hippocampal volume prior to trauma exposure are more likely to develop PTSD, suggesting that some neurological vulnerability exists before a traumatic event ever occurs (Gilbertson et al., 2002). In other words, the nervous system a person brings to a traumatic experience is already shaped by everything that came before it.
Social support is consistently one of the strongest protective factors. A landmark study by Ozer et al. (2003), which analysed data across multiple PTSD studies, found that perceived social support at the time of trauma was among the most robust predictors of whether PTSD developed - more so than the nature of the trauma itself. Dissociation during the event, prior psychological difficulties, and female sex are also associated with higher risk, though none of these factors is deterministic.
What this means in practice is that two people can live through the same event and have entirely different neurological and psychological outcomes. PTSD is not a reflection of how much someone can handle. It is the result of a nervous system doing exactly what nervous systems do - trying to protect you… and sometimes getting stuck in that response.
How the Body Holds Trauma
Trauma is not just stored in the brain - it is held in the body as well. Many individuals with PTSD experience somatic symptoms, such as chronic pain, muscular tension, digestive disruption, an exaggerated startle response - even without conscious memory of the event. These are referred to as somatic markers of trauma.
Research on Holocaust survivors and their descendants has shown that the effects of trauma can extend beyond the individual - altering gene expression in ways that affect how the body regulates stress, and passing those changes to the next generation (Yehuda et al., 2016). This growing field highlights how trauma is not just a psychological experience but can create long-term effects in our bodies.
Healing the Brain After Trauma
Despite the profound effects of trauma, the brain has an incredible ability to heal and rewire itself through a process called neuroplasticity, and this is what makes recovery possible.
Effective trauma treatment tends to draw on both bottom-up and top-down approaches. Bottom-up approaches work through the body first. For instance, somatic therapy and EMDR (Eye Movement Desensitisation and Reprocessing) engage the nervous system directly, processing trauma in a nonverbal, body-based way that bypasses the need to narrate or analyse. Top-down approaches such as CBT or trauma-focused therapy work through cognition, helping individuals reframe their experiences, build coping strategies, and make meaning of what happened.
For many people the most effective treatment combines both.
Conclusion
Understanding the neuroscience of trauma offers both hope and also clarity on why recovery is not simply linear or a matter of willpower. While trauma can lead to significant changes in the brain and body, it can be reversible. Thanks to neuroplasticity, the brain has the remarkable ability to rewire itself, meaning that healing is possible even after profound distress. Research into trauma-informed therapies, such as EMDR, somatic therapy, and cognitive approaches, continues to show promising results in helping individuals process and recover from traumatic experiences.